Blood cancers: everything important to know
BY.
Dr.
FABRIZIO CARNEVALE SCHIANCA
Director of the Center for Stem Cell Transplantation Hemopoietic Stem Cell Transplantation (HSC) and Cellular Therapies
Receiving a diagnosis of blood cancer-also called hematologic, hematopoietic, or oncohematologic disease-or even suspecting it can generate many questions, fears, and uncertainties. These are often complex diseases, with treatment pathways that can be long and require adjustments in daily life. Let’s get some clarity with our expert.
Visita il profilo
The 12 most frequently asked questions about hematologic cancers
1. What is meant by blood cancers?
The term “blood cancers” refers to a group of diseases that affect cells in the blood and lymphatic system.
The main forms are:
- leukemias: mainly affect the bone marrow and blood;
- Lymphomas: they affect the lymphatic system;
- multiple myeloma: involves plasma cells in the bone marrow and can result in bone lesions and impaired renal function;
- Myelodysplastic and myeloproliferativeneoplasms ( affect the bone marrow and impair its blood-producing function (hematopoiesis)
These diseases differ in course and treatment, each with acute/chronic forms and various subtypes, such as Acute Myeloid Leukemia (AML) or Chronic Lymphatic Leukemia (CLL).
2. Are these rare tumors?
Blood cancers are considered relatively rare individually, but as a whole they affect about 30,000 new Italians each year, accounting for about 10 percent of all cancers, with a growing number of people living with these diseases thanks to therapeutic advances that lead to cures in many people and chronicity of the disease in others.
3. What are the most common symptoms of blood cancers?
Symptoms are often nonspecific and may include persistent fatigue, fever, frequent infections, anemia, weight loss, night sweats, or enlarged lymph nodes bone pain. In some cases, diagnosis is made on an occasional basis through routine blood tests.
4. What are blood cancers caused by?
In most cases there is no identifiable cause. Diseases result from acquired genetic alterations that cause cells to proliferate abnormally. Rarely there is a hereditary predisposition.
5. Is it possible to prevent blood cancers?
There are no specific prevention or screening programs. However, paying attention to persistent symptoms and undergoing medical checkups when indicated can aid early diagnosis.
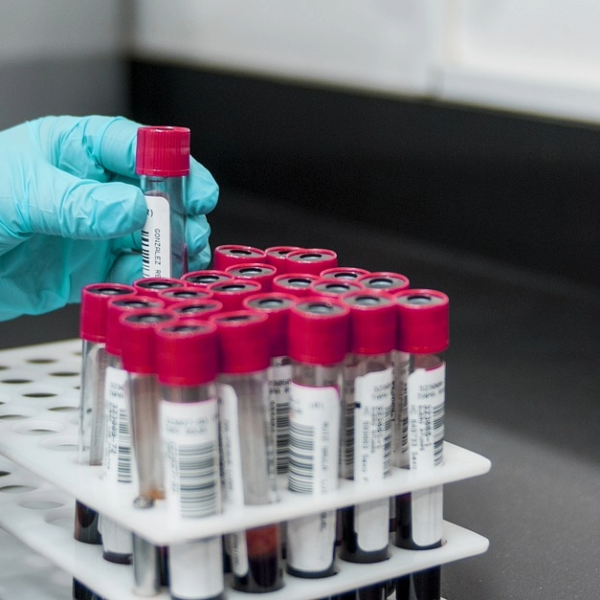
6. How do you arrive at the diagnosis?
The first step is always a thorough medical examination, during which the specialist listens to the symptoms, reconstructs the medical history, and examines the patient. If necessary, they are then requested:
- blood tests;
- Bone marrow biopsy;
- radiological examinations;
- Genetic and molecular testing.
These investigations make it possible to accurately identify the type of blood cancer and build a personalized therapy for that person.
7. What are the main therapies available today?
The main options include:
- chemotherapy;
- Therapies targeting specific molecular alterations;
- immunotherapy;
- Blood stem cell transplantation (from a donor or, in some cases, from the patient himself);
- CAR-T cell therapy, in which the patient’s own lymphocytes (a particular type of white blood cell) are modified in the laboratory to selectively recognize and destroy cancer cells.
Today, treatments are increasingly personalized and targeted to the characteristics of the disease and the patient.
8. How effective is blood stem cell transplantation?
Blood stem cell transplantation is indicated in certain diseases and conditions, but it can be a key therapeutic option with potential for long-term control or cure, thanks to advances in techniques and clinical care.
9. Can a blood cancer be cured?
Many blood cancers today are treatable and curable. Others may be controllable over time. In this second group of diseases we speak of chronic disease, that is, a health disorder that requires periodic visits and protracted treatment (sometimes for many years).
10. How can people live with chronic blood cancer?
Living with a chronic oncohematologic disease means learning how to manage treatment, monitoring, and daily life. A healthy lifestyle, a balanced diet, physical activity compatible with one’s condition, and psychological support can help maintain a good quality of life. Constant dialogue with the treating team is essential to tailor therapies to the patient’s needs.
11. What are the most common side effects of therapies and transplantation?
Side effects vary depending on the treatment and the person. They may include fatigue, nausea, increased risk of infection, hair loss, or changes in appetite. In the case of transplantation, the initial period requires frequent checks. Today, thanks to supportive therapies, many side effects are preventable or effectively manageable.
12. Why turn to a specialized center such as the Candiolo Institute IRCCS?
A referral center such as the Candiolo IRCCS Institute guarantees a highly specialized approach to oncohematologic diseases, based on integrated multidisciplinary expertise and an organization dedicated to the management of complex diseases.
The patient is taken care of by a team composed of oncologists, hematologists, anatomo-pathologists, molecular biologists, radiologists, and support specialists, who are able to define individualized diagnostic and therapeutic pathways.
The Institute also provides access to innovative therapies and clinical research, with the opportunity to participate in clinical trials, which are critical to making innovative treatments available under safe and appropriate conditions.
An additional distinguishing feature is advanced molecular characterization diagnostic protocols, which enable the application of precision medicine principles, identifying specific biological alterations in the disease and guiding the choice of different treatment strategies such as molecular-targeted therapies.
Alongside these approaches, the Institute has always been a leading player in the development and use of immunological and cellular therapies, including allogeneic blood stem cell transplantation and CAR-T therapies. These strategies represent one of the greatest innovations in onco-immunology today, because they allow the patient’s immune system to be “trained” to recognize and highly selectively target cancer cells through specific targets (antigens).
All of this must take place within structured care pathways that pay attention not only to disease control but also to the patient’s quality of life during all phases of treatment and recovery at the end of care.